
 |
|
Bios Dr. Arjmand practices at the Mississauga Retina Institute in Toronto. |
In the ever-shifting landscape of medical retina, the introduction of faricimab represents a significant stride forward. Approved by the FDA and Health Canada in January and May 2022, respectively, this new therapy has garnered attention due to its longer durability in comparison to its predecessors within the anti-VEGF class, while maintaining a similar safety profile.
As we delve into the initial real-world experiences with faricimab, valuable practical insights and challenges have emerged, shedding light on nuances with its administration in the clinic, as well as the promising potential it holds for patients dealing with diabetic macular edema and neovascular age-related macular degeneration.
Faricimab (6 mg/0.05 mL) (Vabysmo, Genentech/Hoffman La Roche) is a humanized monoclonal antibody with bispecificity to VEGF-A and Ang-2. The VEGF-A pathway inhibition impedes endothelial cell proliferation and neovascularization, while Ang-2 blockade reinforces anti-VEGF signaling cascades and increases vascular stability.1,2 It’s currently approved for treatment of patients with nAMD and DME with the option for treatment from one to four months apart in the first year following an initial once monthly loading dose for four months.
The real world vs. clinical trials
Like prior classes of anti-VEGF drugs, the product monograph instructions for Faricimab may differ from practical considerations outside of clinical trials.
•Although patients can be extended up to 16 weeks between doses, the product monograph instructs visual acuity and anatomic evaluations at weeks “20 and 24 to inform dosing at intervals of eight, 12 or 16 weeks through week 60.”2,3 While these instructions may well apply to treatment-naïve patients, in the real world, many “switch” patients agree to start on faricimab on the premise that they would have fewer visits to the clinic. Acuity and OCT imaging at extra monthly intervals after the loading dose isn’t practical in the real world.
•Most early adopters of faricimab may choose to switch two classes of patients who aren’t the primary focus of clinical trials. The first group includes patients who need anti-VEGF therapy every four to six weeks. The second group are suboptimal responders with persistent intraretinal or subretinal fluid despite monthly treatments. TENAYA, LUCERNE, YOSEMITE and RHINE all primarily recruited treatment-native patients; however, only 25 percent of those in YOSEMITE and RHINE comprised switch patients.2,3 As such, loading and dosing data for this class of patients isn’t yet well-guided by evidence.
•There are several differences in the administration of the drug in clinical trials versus in the real world. The drug monograph for faricimab indicates that the procedure must be carried out under aseptic conditions with the use of surgical hand disinfection, sterile gloves, drape and a sterile speculum.1 Meanwhile, the most recent ASRS PAT survey indicates that most specialists in the United States and Canada use a clean but not aseptic technique for intravitreal injections in the clinic. As well, many have moved away from the use of speculums, which may cause additional discomfort, corneal abrasions and sensitivity post-procedure. Most specialists now use cotton-tip applicators or fingers to keep the lid margin away from the injection site.
•While many of our patients in the real world require bilateral, same-day, anti-VEGF treatment, bilateral use hasn’t been studied in the trials.
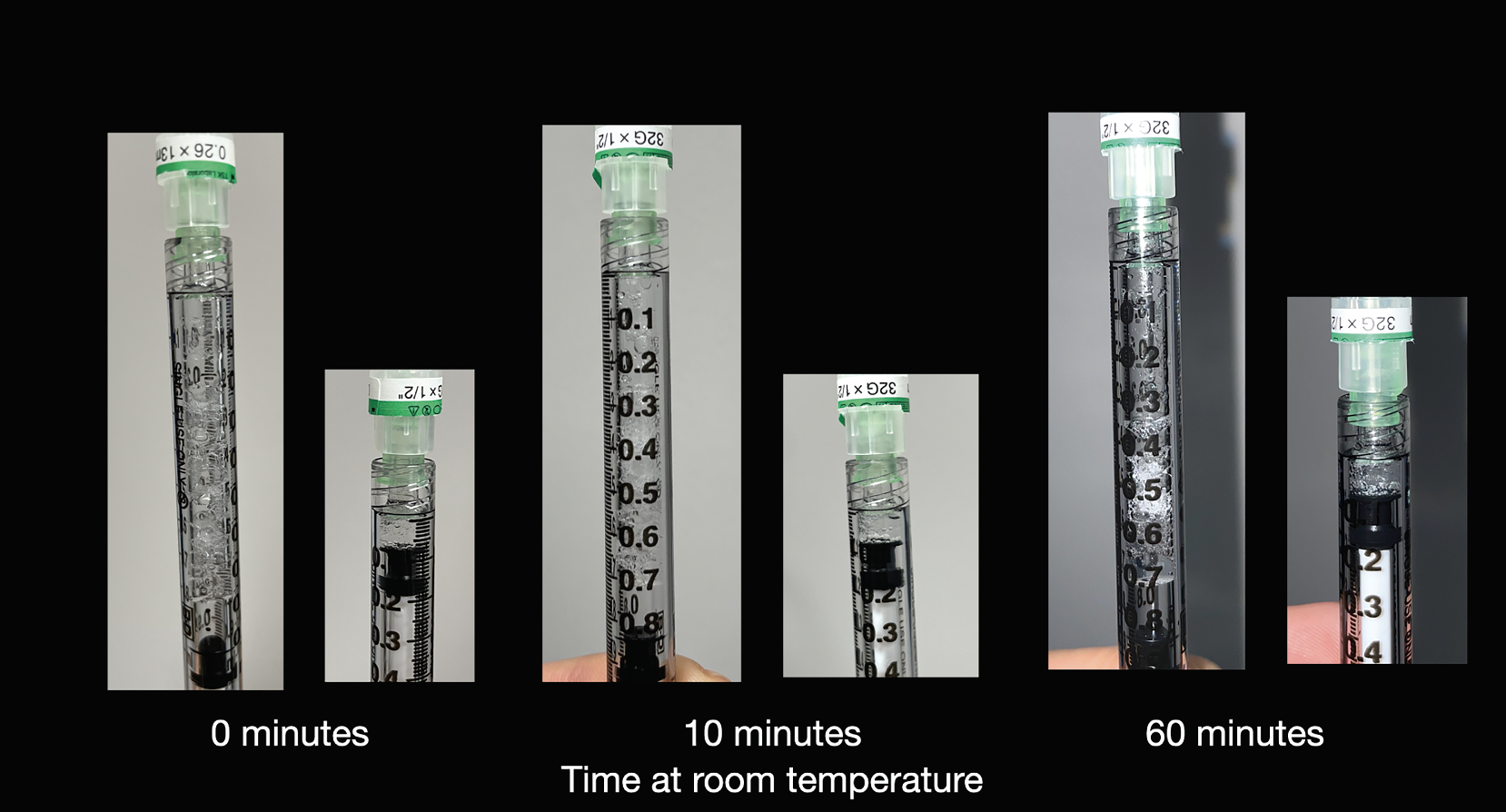 |
| Figure 1. Three vials of faricimab drawn up in a Luer-lock 1 mL syringe before and after priming to 0.05 mL. Faricimab drawn up from the vial taken immediately out of the fridge (left), kept at room temperature for 10 minutes (middle) and 60 minutes (right). No discernable difference was noted in the number of bubbles, the number of times the syringe had to be tapped, ease of priming the syringe or the speed of injection. |
Thoughts on drug handling
As busy retina specialists, we may not always have time to carefully examine the product monographs for medications we administer in the clinic. Faricimab shouldn’t be injected while it’s cold. Instead, it should be warmed to room temperature (~25 degrees C/77 F) and is deemed stable at room temperature for up to 24 hours.1
In our practice, anti-VEGF medications (ranibizumab/Aflibercept) are often taken out at the beginning of the day and kept on ice until used. As we currently have fewer patients on routine faricimab injections on any injection day, this drug often gets taken out of the fridge a few minutes before its use. To warm up the drug, one could keep the vial in a scrub/white coat pocket for a few minutes prior to use. However, it should also be kept still on a flat surface prior to drawing up the medication to minimize bubbles.
It’s been anecdotally speculated that, at room temperature, the drug will be more easily drawn up with fewer trapped air bubbles. We put this hypothesis to the test, comparing three vials of faricimab. All variables were the same except for the duration of time the drug was left at room temperature. Vial 1 was taken out of the refrigerator and immediately drawn up into a TB syringe. Vial 2 was kept at room temperature for 10 minutes prior to being drawn, and vial 3 was kept at room temperature for an hour prior to being drawn. The same physician performed the procedure all on three vials. There was no visible difference in the volume of trapped air bubbles, the number of times the syringe had to be tapped to let out the trapped air bubbles, ease of priming the syringe or the speed of injection. (See Figure 1)
Faricimab’s introduction into the treatment arena for DME and nAMD represents a significant advancement and comes with unique challenges in the real-world clinical setting. The application of this therapy may diverge from clinical trial protocols in several key aspects, such as patient selection, dosing intervals and administration techniques. These variations necessitate a flexible and patient-centered approach in clinical practice. Additionally, practical considerations, such as the proper warming and handling of the medication, are crucial for effective administration. Our experience underscores the importance of adapting and refining clinical practice to bridge the gap between the controlled trial setting and the dynamic nature of everyday clinical care. RS
REFERENCES
1. Hoffman-La Roche Limited. Product Monograph Including Patient Medication Information, Vabysmo Faricimab injection, Single-use vials, 6 mg/0.05 mL solution for intravitreal injection, Professed Standard, Ophthalmological/ Anti-vascular endothelial growth factor and anti-angiopoietin-2 agent. Mississauga, Ontario, Canada. May 27, 2022. [cited Oct 9 2023]. https://pdf.hres.ca/dpd_pm/00066073.PDF.
2. Heier JS, Khanani AM, Quezada Ruiz C, Basu K, Ferrone PJ, Brittain C, Figueroa MS, Lin H, Holz FG, Patel V, Lai TYY, Silverman D, Regillo C, Swaminathan B, Viola F, Cheung CMG, Wong TY; TENAYA and LUCERNE Investigators. Efficacy, durability, and safety of intravitreal faricimab up to every 16 weeks for neovascular age-related macular degeneration (TENAYA and LUCERNE): Two randomised, double-masked, phase 3, non-inferiority trials. Lancet. 2022;19:399:10326:729-740.
3. Wykoff CC, Abreu F, Adamis AP, Basu K, Eichenbaum DA, Haskova Z, Lin H, Loewenstein A, Mohan S, Pearce IA, Sakamoto T, Schlottmann PG, Silverman D, Sun JK, Wells JA, Willis JR, Tadayoni R; YOSEMITE and RHINE Investigators. Efficacy, durability, and safety of intravitreal faricimab with extended dosing up to every 16 weeks in patients with diabetic macular oedema (YOSEMITE and RHINE): Two randomised, double-masked, phase 3 trials. Lancet. 2022;19:399:10326:741-755.



