
 |
Bios Dr. Guiseppi is an ophthalmologist in Galveston, Texas. Dr. MomPremier is a vitreoretinal specialist at the MomPremier Eye Institute, Desoto, Texas. DISCLOSURES: The authors have no financial disclosures. |
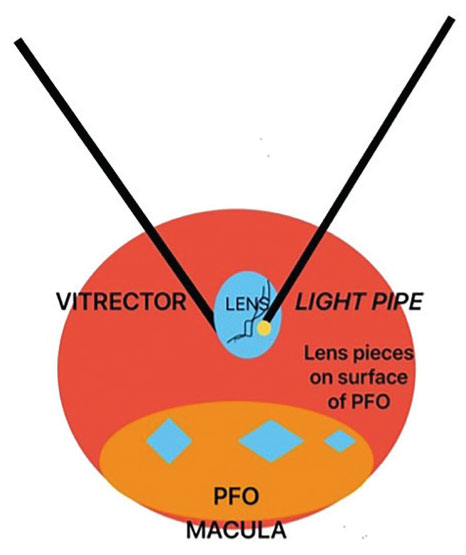
A partial perfluoro-n-octane (PFO) fill before performing lensectomy is a useful tool to protect the macula and peripheral retina from unintentional trauma during lensectomy, because the large mobile irregular lens pieces may fall at a high velocity onto the macula multiple times.
Perfluorocarbon liquids have been shown to potentially shield the macula from the impact of dropped intraocular foreign bodies by deflecting the trajectory on the perfluorocarbon liquid-balanced salt solution interface.1
Our case
In the accompanying video, we operate on a middle-aged man who had a subluxed lens after blunt force trauma. We used a 23-gauge vitrector set for pars plana lensectomy with a bimanual technique to break the lens into smaller pieces, which helped to make the lensectomy more efficient (Figure).
We used the light pipe to directly apply mechanical pressure onto the lens surface and feed it into the vitrector and break it into smaller pieces. Smaller pieces were easier to remove, sometimes with just aspiration from the vitrector.
Intraoperative troubleshooting
In patients with a medium-density lens, we recommend initiating the lensectomy with the larger vitrector and reserving the phacofragmatome for very dense lenses.
A core vitrectomy, posterior vitreous detachment induction and a good peripheral vitrectomy before starting the pars plana lensectomy are also key. During lensectomy, a loss in aspiration suggests that lens pieces may be occluding the vitrector, so it’s important to flush the vitrector line outside the eye.
 |
|
We do bimanual pars plana lensectomy using the vitrector and light pipe. The light pipe can help to feed larger lens pieces into the vitrector. The perfluoro-n-octane bubble protects the macula from mobile lens pieces during the procedure. |
Using PFO
We applied intraoperatively about 2 to 3 mLs of PFO (Perfluron, Alcon) to cover the posterior pole to the arcades, including the macula. Once we aspirated the large lens pieces, we safely removed the PFO and placed a secondary intraocular lens.
A scleral depressed exam at the end of the case ensured that no peripheral retinal breaks were present.
PFO may be costly and isn’t necessary for all cases of pars plana lensectomy, but we recommend considering it in cases when the lens is dense and may fall multiple times onto the macula during surgery
Bottom line
Instilling and removing PFO is an additional but useful step in pars plana lensectomy by preventing iatrogenic damage to the macula during these cases. We recommend taking these additional steps for the entire lens or large lens pieces. RS
REFERENCES
1. Rejdak R, Choragiewicz T, Moneta-Wielgos J, et al. Intraoperative macula protection by perfluorocarbon liquid for the metallic intraocular foreign body removal during 23-gauge vitrectomy. J Ophthalmol. 2017:6232151.



